
The Dobbs decision, one year later
Twelve months after the US Supreme Court decision, we reflect on the impact the overturning of Roe v. Wade has had on women with breast cancer.
- 06/23/23

One year ago, Living Beyond Breast Cancer issued a statement, joined by eight partners, to express our grave concerns about the implications of the US Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization on the breast cancer community.
This ruling overturned the 50-year precedent of Roe v. Wade and put decisions about a woman’s right to a safe medical abortion into the hands of state legislators. Today, we have ample evidence from physicians and women across the nation that confirms our fears. In the new legal landscape, evidence-based care is compromised, physicians are stymied, and women’s medical options are severely limited. We acknowledge not everyone shares our view, and we continue to stand with the majority of US doctors and medical groups that have deep concerns about the implications of this ruling.
On this anniversary of the Dobbs decision, I want to share with you what we have learned, through the stories doctors and women have shared with us.
Treatment obstacles and delays
Put yourself in the shoes of Tanya (we are not using her real name, per her request), a premenopausal woman who was diagnosed with de novo breast cancer metastases to the lung, liver, and brain. After having local therapy, she experiences a complete response to systemic treatment, showing no measurable disease for two years. Filled with hope, she falls in love and marries.
But at age 48, Tanya finds herself with an unplanned, unwanted pregnancy, living in a state where abortion is banned. Her highly effective treatment is potentially toxic to a fetus and could induce an abortion, so her doctor must stop it immediately. Tanya cannot afford travel to another state. For almost three months she is unable to receive the medication that has been keeping her cancer at bay. Finally, a legal solution is found, but Tanya has been without cancer treatment for one-quarter of a year, and both she and her doctor are profoundly worried about the consequences.
Dangerous trends come together
We at LBBC celebrate advances in medicine that have given many women the option to continue pregnancies and deliver healthy babies during breast cancer treatment. We spoke up for moms during the infant formula crisis. However, the overlapping trends of decreasing age at first breast cancer diagnosis and increasing age of childbearing have created a dangerous scenario. Cancer affects 1 in 1,000 pregnancies in the US, and approximately 1,500 women each year will have a breast cancer diagnosis and a pregnancy simultaneously.
In addition, many new and improved treatments—like targeted therapies for HER2-positive cancers and immunotherapies for triple-negative breast cancer—are toxic to fetuses. The gap between what can be done to save women, and what is safe to do during pregnancy, grows wider all the time.
The question now is: Who should decide what path a woman takes when optimal cancer care is in conflict with carrying a pregnancy to term?
We stand with patients
At LBBC, we believe in each person’s right to make medical decisions based on scientific evidence, with guidance from their healthcare team, steeped in their own beliefs, priorities, and values. Clear, transparent communication between patients and physicians deserves privacy and respect.
Over the past 12 months we have seen one state after another erect huge, sometimes insurmountable, barriers to safe medical abortion. LBBC Medical Advisory Board member Virginia F. Borges, MD, MMSc, director of the Young Women’s Breast Cancer Translational Program at the University of Colorado Cancer Center, told me that the wording of state statutes regarding legal exceptions for abortion is vague and confusing. Developed by legislators rather than physicians, these laws are not rooted in clinical knowledge that accounts for the long-term implications of altering cancer treatment. This leaves many physicians in “a state of chaos,” subject to ethical and legal uncertainties.
With such uncertainty, clinicians will fear criminalization and may not act in the best interest of the patient.
In states where abortion is outlawed, or permitted only during the weeks when most women are not even aware they are pregnant, many physicians fear for their licenses and their lives if they want to offer optimal cancer care to their patients.
Current status of abortion laws by state
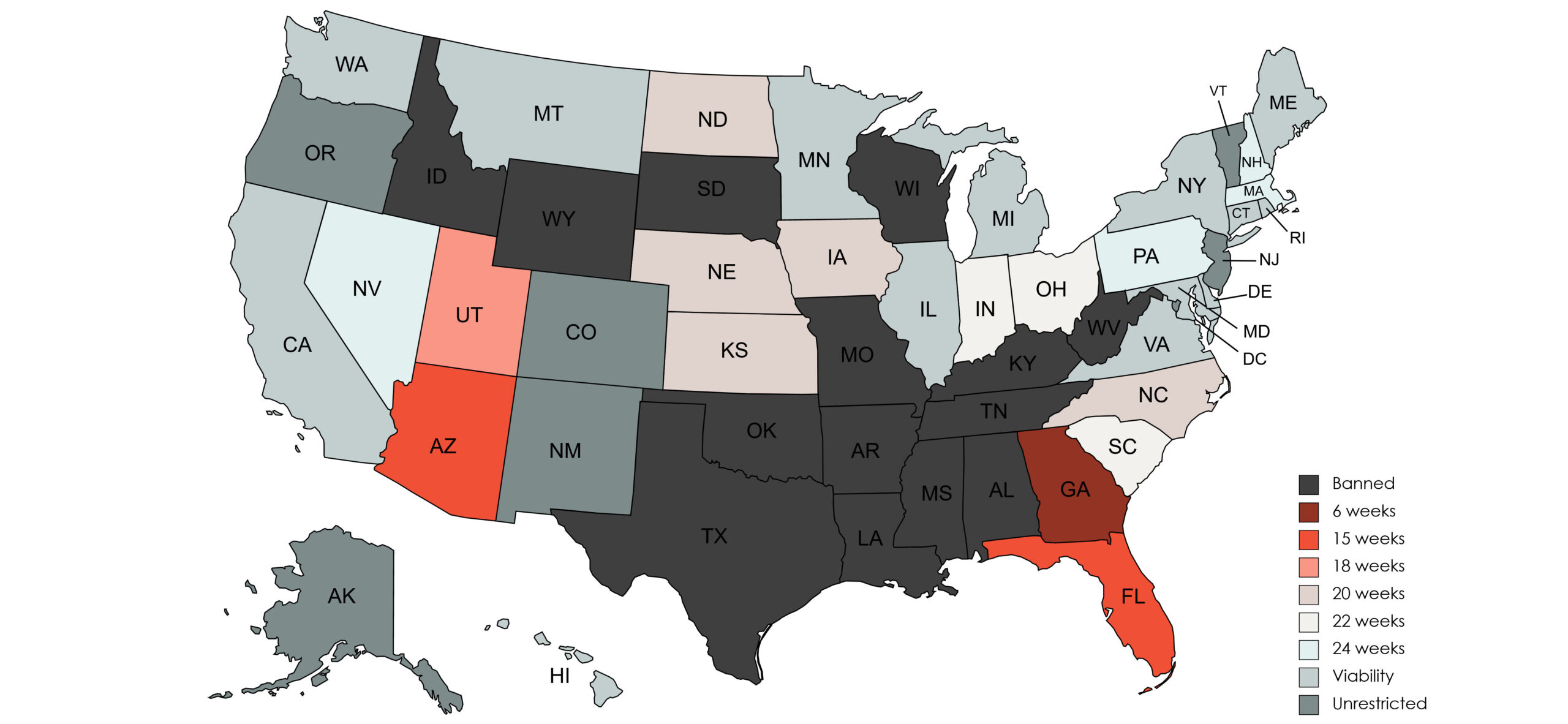
Sources: US News and World Report, Guttmacher Institute, ProPublica, Center for Reproductive Rights, Accessed April 9, 2023
Credit: Map courtesy of Virginia F. Borges, MD, MMSc
Dr. Borges and other physicians told me of situations in which trying to save the mother and bring the pregnancy to the point of viability ended in disaster for both. Or a baby was born, only to lose its mother to cancer in a matter of months.
Managing pregnancy during cancer treatment requires a specialized team of high-risk obstetric experts. Yet large portions of the nation have what Dr. Borges calls “maternal health deserts.” Society does not provide the type of comprehensive medical care for most women that these laws demand.
Choice is imperative, delay is deadly
As we enter the second year after Dobbs, LBBC continues to wholeheartedly support people’s ability to make decisions about their own bodies. We continue to believe that medical decisions are personal and private, to be made between people with cancer and their doctors. Of all the women who find themselves pregnant with breast cancer, 9-28% will choose to terminate the pregnancy (resources here). But confusion and delay do not benefit anyone. In fact, a 2020 meta-analysis showed that the mortality risk among patients with cancer increased by as much as 13% with every month that treatment was postponed.
Our organization has long been a leader in creating programs, services, and safe community spaces for young women impacted by breast cancer. We understand that, in the words of Dr. Borges, “therapeutic decision making for patients with breast cancer is complex and multidisciplinary, involving various modes of treatment including surgery, systemic therapies like chemotherapy and hormone suppression, and radiation.” We oppose any legislation or policy that is not based in science, respecting the rights, health, and well-being of every individual, and that interferes in the private communications between people and their physicians.
Learn more
- What Dobbs means for patients with breast cancer (New England Journal of Medicine)
- Lack of access to abortion has had an impact on cancer care (Cancer Therapy Advisor)
- How strict abortion laws are delaying cancer treatment (Healthline)
Get involved
More Recent News
- Research points to better testing, new treatment options across breast cancer types | ASCO 2026
- Ready for action in survivorship: Reducing risk of recurrence and improving quality of life | ASCO 2026
- Pivotal progress in triple-negative breast cancer | ASCO 2026
- Unpack your worries: Making the most of travel with breast cancer
Advocacy in Action
- Claudia De Pasquale makes herself whole with reconstruction choices
- Lighting a path from survival to healing after breast cancer
- From self-focus to community care: Lisa Walker’s life after breast cancer
- Beyond basketball: Family transforms great loss into a legacy of support for breast cancer
Advocacy opportunities
Stay connected
Sign up to receive emotional support, medical insight, personal stories, and more, delivered to your inbox weekly.

- Joined LBBC in 1996 when she became the organization’s first executive director; she was named CEO in 2008
- Increased LBBC’s annual budget from $100,000 to over $8,000,000
- Founding member of the Metastatic Breast Cancer Alliance
- Secured 4-star rating, the highest available rating, from Charity Navigator for 20 consecutive years in recognition of LBBC exceeding industry standards
- Spearheaded the effort for LBBC to be the Breast Cancer Lead Organization for No One Missed, a national campaign to raise awareness of biomarker testing
- Inspired by her mother’s courage and outrage after being diagnosed with breast, uterine, and ultimately passing away from lung cancer in 2010
Tagged:

Living Beyond Breast Cancer is a national nonprofit organization that seeks to create a world that understands there is more than one way to have breast cancer. To fulfill its mission of providing trusted information and a community of support to those impacted by the disease, Living Beyond Breast Cancer offers on-demand emotional, practical, and evidence-based content. For over 30 years, the organization has remained committed to creating a culture of acceptance — where sharing the diversity of the lived experience of breast cancer fosters self-advocacy and hope. For more information, learn more about our programs and services.